
What General Practitioners Should Know About Shelter Animals
(A clinical reference for first-contact veterinary care)
Shelter standards are important resources outlining both the minimum acceptable and the ideal practices for housing, husbandry, and medical and behavioural care in animal shelters. These guidelines are designed to be relevant and adaptable for all types of organizations, while simultaneously outlining a minimum standard that all organizations must aim to reach regardless of resource limitations. There are now many self-assessment tools that accompany the guidelines and allow organizations to identify areas for improvement or to use as a part of shelter consultations. The following outlines a number of guidelines and position statements for Shelter Standards in North America.
SECTION 1 — Treating Animals Returning to a Shelter or Foster Home
When an animal will be returning to a shelter or foster home rather than a permanent home, treatment plans need to reflect the realities of those environments.
- Foster homes vary considerably in experience. Some fosters are seasoned medical volunteers comfortable with pills, injections, and complex protocols; others are first-time caregivers. Unless you know the foster’s capabilities, apply the same conservative assumptions as you would for a shelter — and when in doubt, check with the shelter’s foster coordinator before prescribing.
- Most shelters have staff present for only 8–12 hours a day, so prescribe medications that can be given once or twice daily at most. Three- or four-times-daily dosing is not feasible and sets the animal up for missed doses or treatment abandonment.
(Important: The shelter is the client — the foster home is acting as the animal’s agent/caregiver onthe shelter’s behalf. Most foster homes do not have authority to authorize treatment, agree to costs, or make medical decisions independently. Significant clinical decisions — diagnostics, procedures, medications beyond routine care — should be approved through the shelter directly, not the foster. When in doubt, call the shelter before proceeding.) - Choose low-stress administration routes whenever possible. Liquid medications are generally easier to give than pills in a shelter setting, and flavored formulations are meaningfully better than bitter ones for animals that aren’t highly food-motivated or easily handled. Reducing the stress of each treatment matters both for the animal’s wellbeing and for staff and volunteer compliance.
- Recognize that the “ideal” treatment may not be realistic — financially or practically. Shelters operate under significant resource constraints, and a technically superior treatment that cannot be consistently administered is worse than a good-enough treatment that can. Lead with the highest-value interventions: the ones most likely to make a real difference given the constraints. If you are uncertain what a shelter can support, ask.
SECTION 1 — Treating Recently Adopted Animals
Medical Records
Adopters are sent home with a copy of their animal’s shelter medical records and are instructed to bring them to their first veterinary visit. If a client arrives without records or the records seem incomplete, the records exist — contact the shelter directly by phone or email to obtain them.
Unknown History and Age Estimation
Stray and owner-surrendered animals frequently arrive with no known history. Age is estimated based on dentition and physical condition and should be understood as an approximation, not a confirmed birth date.
Vaccines
Shelter vaccine protocols differ from private practice in meaningful ways. Vaccines are started earlier and given more frequently because disease exposure risk is significantly higher in a congregate setting. Core vaccines and rabies are typically administered at or after 12 weeks of age per ASV guidelines — but many kittens and puppies are adopted out before 12 weeks and will not yet have received a rabies vaccine. This is expected and normal, not an oversight.
| One point that surprises many clinicians: a killed rabies vaccine can safely be given within two weeks of an adjuvanted or recombinant vaccine. There is no need to delay. |
Spay/Neuter
Pediatric spay/neuter (performed at 8–16 weeks) is common practice in shelters and is safe. A tattoo at the incision site is standard and indicates the animal has been altered — do not mistake it for an injury or marking of unknown origin.
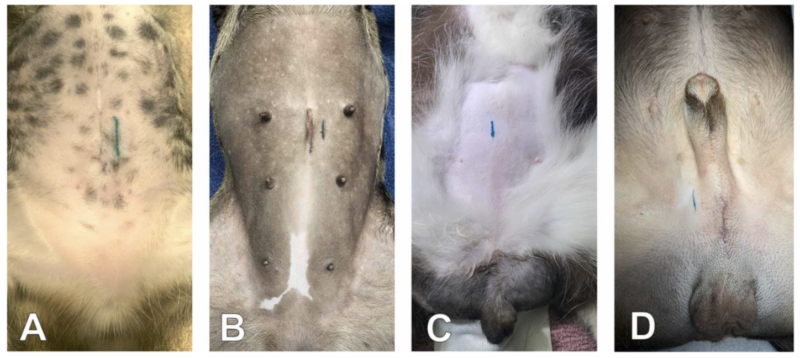
(Image and caption from Mielo, Amirian, & Levy, 2022).
Community cats (feral and free-roaming) will have an ear tip — the tip of the left ear is surgically removed while the animal is under anesthesia. This serves as a universal visual indicator of sterilization and previous trapping.

Microchipping
Nearly all shelter animals are microchipped prior to adoption. Encourage clients to register and keep their contact information current in the microchip database — this is one of the highest-yield reminders you can give at a first visit.
Upper Respiratory Infections
URIs are extremely common in some shelter environments. In cats, the vast majority are caused by feline herpesvirus (FHV-1) and, to a lesser extent, calicivirus. Canine infectious respiratory disease complex (CIRDC) in dogs is often viral, and bacterial infection should not be assumed to be present in all cases.
Stress is a major trigger for herpesvirus reactivation — a newly adopted cat showing URI signs in the first days to weeks at home is most often experiencing stress-induced shedding, not a new infection acquired post-adoption. Manage expectations with new adopters accordingly and treat symptomatically.
Antibiotics should not be prescribed routinely, as these infections are frequently viral and/or self-limiting. Mycoplasma and Chlamydia are common secondary infections in cats; Bordetella is common in dogs. When antibiotics are indicated, they should target these organisms — doxycycline is first-line in shelter medicine.
If a patient has come from a shelter with a high incidence of URI, husbandry factors are worth flagging. Upper respiratory infections were once considered an inevitable part of shelter life but are largely preventable through appropriate housing, capacity management, and stress reduction.
FIV/FeLV and Heartworm Testing
Not every cat leaving a shelter has been tested for FeLV/FIV, and this is intentional. The ASV guidelines do not recommend universal testing — it is based on individual animal risk and shelter resources. Do not assume a lack of testing indicates negligence. Heartworm testing practices similarly vary by shelter and region.
FIV-positive cats can be housed with FIV-negative cats provided the cats are not fighting. FIV is transmitted primarily through deep bite wounds; casual contact such as shared food and water bowls, grooming, and litter boxes does not present a meaningful transmission risk. An FIV diagnosis is not, on its own, a reason to separate cats or to decline adoption into a multi-cat home.
Behaviour: Decompression and the 3-3-3 Rule
Shelter behaviour often does not reflect an animal’s true temperament. Animals in a kennel environment are stressed, suppressed, or hypervigilant — what you see is not a reliable baseline. Counsel new owners to expect a structured decompression period, commonly described as the 3-3-3 rule.
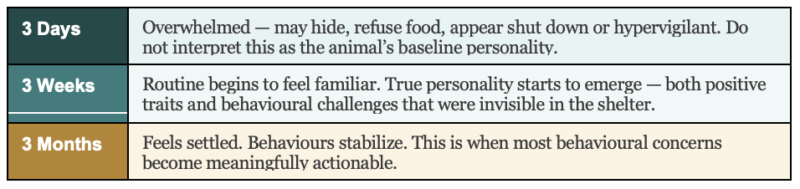
Behaviours commonly masked in the shelter and emerging only after adoption include separation anxiety (absent in the kennel, triggered once a bond forms), resource guarding, leash reactivity, multi-pet conflict, and in cats, stress-related marking or spraying. Owners should be advised not to judge behaviour in the first two to four weeks and to allow the animal to explore and settle at its own pace.
Some animals leaving the shelter will have been on medications — gabapentin, trazodone, or other anxiolytics — prescribed to manage kennel stress or facilitate handling. These may no longer be necessary once the animal is in a calm home environment and should be weaned gradually rather than stopped abruptly. Review the discharge records or contact the prescribing veterinarian to confirm what was given, at what dose, and for how long before making changes.
SECTION 2 — Treating Animals Returning to a Shelter or Foster Home
When an animal will be returning to a shelter or foster home rather than a permanent home, treatment plans need to reflect the realities of those environments.
- Most shelters have staff present for only 8–12 hours a day, so prescribe medications that can be given once or twice daily at most. Three- or four-times-daily dosing is not feasible and sets the animal up for missed doses or treatment abandonment.
- Foster homes vary considerably in experience. Some fosters are seasoned medical volunteers comfortable with pills, injections, and complex protocols; others are first-time caregivers. Unless you know the foster’s capabilities, apply the same conservative assumptions as you would for a shelter — and when in doubt, check with the shelter’s foster coordinator before prescribing.
| Important: The shelter is the client — the foster home is acting as the animal’s caregiver on the shelter’s behalf. Most foster homes do not have authority to authorize treatment, agree to costs, or make medical decisions independently. Significant clinical decisions — diagnostics, procedures, medications beyond routine care — should be approved through the shelter directly, not the foster. When in doubt, call the shelter before proceeding.d to delay. |
- In cats, liquid medications are generally easier to administer than pills. Reducing the stress of each treatment matters both for the animal’s wellbeing and for staff and volunteer compliance.
- Recognize that the “ideal” treatment may not be realistic — financially or practically. Shelters operate under significant resource constraints, and a technically superior treatment that cannot be consistently administered is worse than a good-enough treatment that can. Lead with the highest-value interventions: the ones most likely to make a real difference given the constraints. If you are uncertain what a shelter can support, please ask.
Additional Resources
ASV Guidelines for Standards of Care in Animal Shelters (2022): https://jsmcah.org/index.php/jasv/issue/view/2
WSAVA 2024 Vaccination Guidelines for Dogs and Cats: https://wsava.org/global-guidelines/vaccination-guidelines/
Koret Shelter Medicine Program — Neonatal Vaccination Recommendations: https://www.sheltermedicine.com/library/resources/neonatal-vaccination-recommendations
Mielo, M. R., Amirian, E. S., & Levy, J. K. (2022). Identification of spayed and neutered cats and dogs: Veterinary training and compliance with practice guidelines. The Veterinary Journal, 285, 105856. https://doi.org/10.1016/j.tvjl.2022.105856
CASCMA Website: https://www.cascma.org